
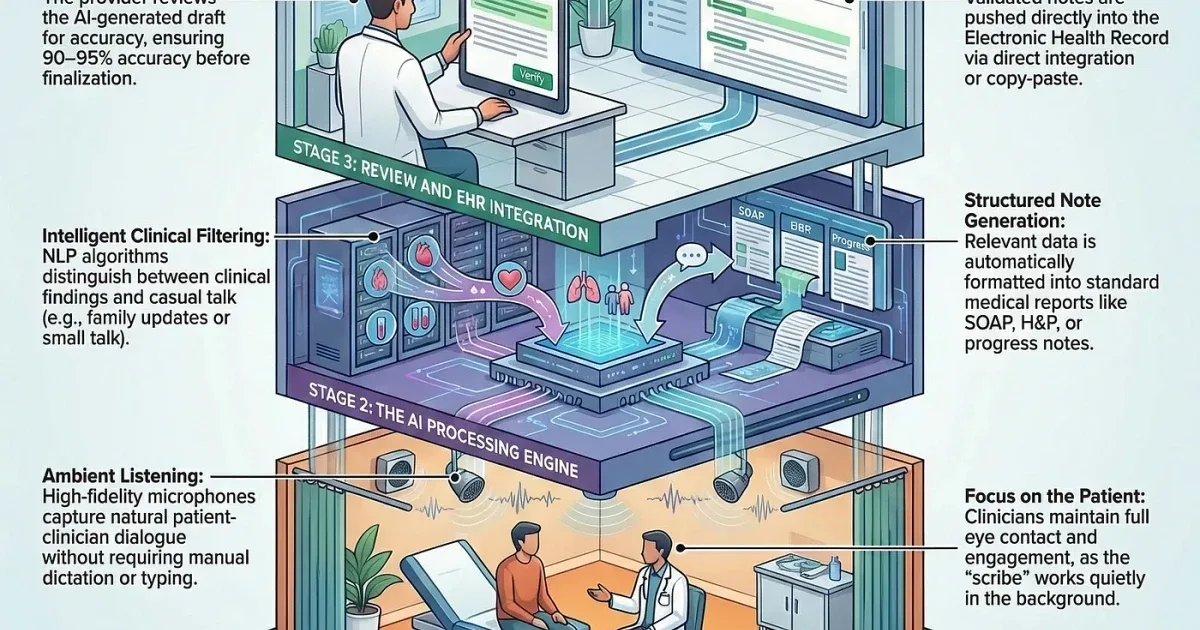
Medical clinics are rapidly integrating ambient AI scribes to automate clinical note-taking, promising to ease physicians’ administrative burdens and allow more direct patient interaction. These AI tools use live audio capture during consultations to generate electronic health record (EHR) summaries, which clinicians can review and finalize. However, the presence of microphones in exam rooms is raising significant questions about patient consent, the accuracy of the documentation, and ongoing liability.
The technology aims to eliminate the extensive time doctors spend charting by automatically transcribing conversations, symptoms, medications, and consent details. A prominent example, Medscape’s Scribe product, operates exclusively in the U.S. and claims compliance with privacy standards, deleting transcripts and summaries after a limited retention period. Despite these safeguards, errors remain a critical concern. Misinterpretations by the AI—such as incorrect medication names or distorted symptom explanations—risk introducing mistakes into patients’ medical records, potentially affecting future care.
Ultimately, responsibility for the accuracy of the medical chart stays with the clinician even when AI drafts the initial note. This has sparked legal scrutiny. A class-action lawsuit filed against Sharp HealthCare in California alleges the use of an ambient AI documentation tool without proper patient consent and incorrectly recorded consent in medical records. This case highlights how AI’s swift adoption contrasts with slower developments in regulatory and policy frameworks governing these technologies.
A quality-improvement study published in JAMA Network Open evaluated experiences among pilot users, involving both clinicians and patients. The majority of consent processes involved verbal discussions before the visits, but patient comfort varied depending on their trust in the clinician and understanding of the AI’s function. Participants expressed a desire for enhanced transparency and more flexible consent options, including educational materials, digital support, assistance from nonclinical staff, and the ability to opt out of AI recording.
The efficiency gains are considerable. The American Medical Association reported that The Permanente Medical Group used ambient AI scribes over two million times within a year. Kaiser Permanente noted that this technology saved thousands of documentation hours over just over a year, translating into nearly 1,800 workdays reclaimed. Physicians also reported improved communication with patients thanks to reduced screen time and more face-to-face engagement.
Yet, alongside these benefits, the integration of ambient AI scribes introduces new complexities. Clinics and health systems must balance innovation with safeguarding patient confidentiality and ensuring accurate, legally sound medical records. Awareness and robust policies surrounding AI use in clinical documentation remain critical as this technology becomes more widespread.